

At our center, we offer a comprehensive range of diagnostic and minimally invasive surgical procedures to accurately identify underlying causes of infertility and enhance the chances of successful conception.

A minimally invasive, day-care procedure performed under short anesthesia. A small incision is made near the navel through which a camera is introduced to visualize the uterus, fallopian tubes, ovaries, and surrounding pelvic structures.
Cryopreservation is the process of preserving sperms, excess embryos, blastocysts and more recently oocytes in a frozen state for future retrieval and usage. It requires sophisticated, expensive and computerized equipments for the procedure and liquid nitrogen jars for storage. It also requires special media formulated for freezing technique.
The excess oocytes, embryos and sperms are initially exposed to cryoprotective agents in order to dehydrate them, followed by loading into straws, slow cooling and finally plunging into a temperature of – 196°c in liquid nitrogen where it can be preserved indefinitely (ideally a clinic is allowed to store for a period of 5 years before it can decide the next best approach)
Cryopreservation is very useful for those patients who have hyperstimulation syndrome and have excess oocytes or embryos requiring storage for future use. It is also used for the male partner to freeze semen samples ahead of the procedures giving them flexibility where jobs are concerned. We also freeze ahead of procedures in those whom a collection problem is anticipated or for using pooled samples in case of male factor. At our centre we mostly freeze embryos in the pronuclear stage.
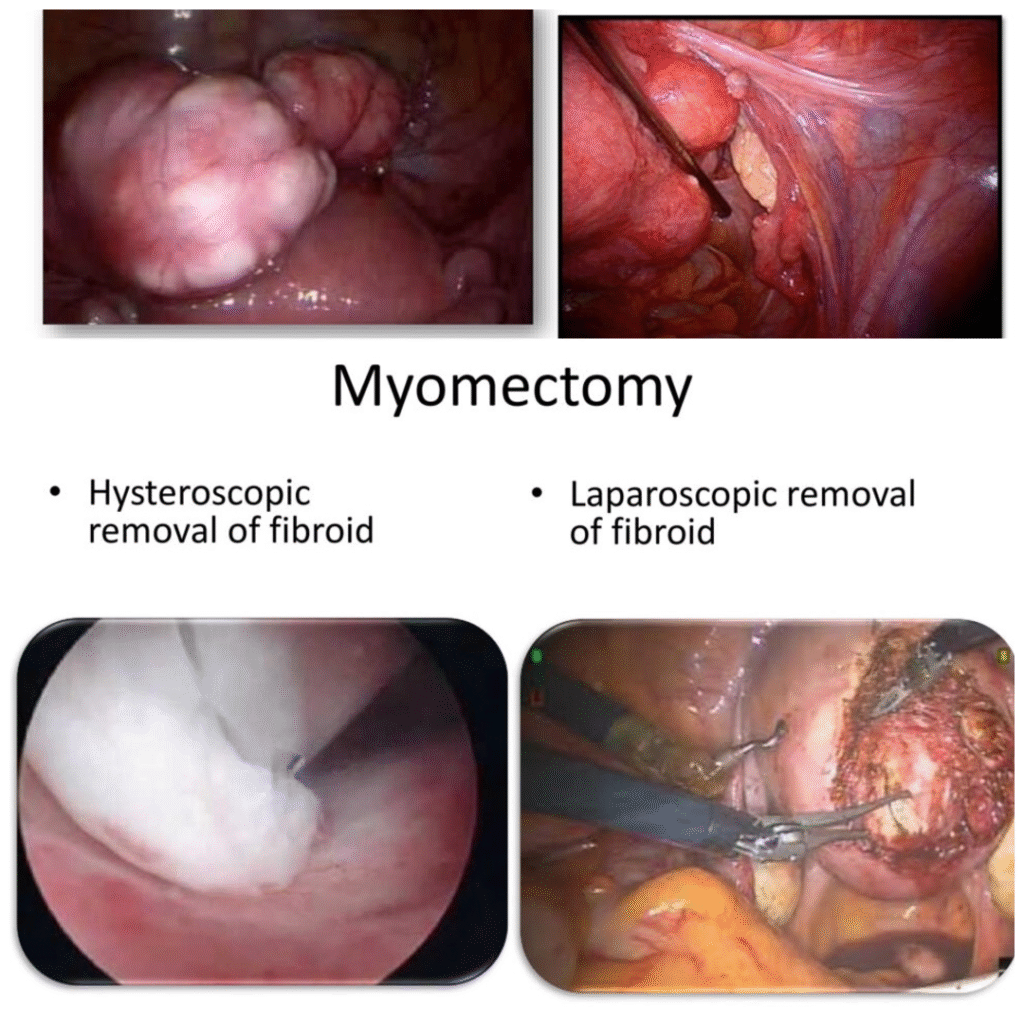
Fibroids are benign tumors arising from the uterine musculature. They are hormone dependant and have a tendency to grow. Sometimes these tumors due to their size and location tend to interfere with normal fertility. Hence their removal either laparoscopically or by an open surgery (laparotomy) improves chances of conception. The decision of assessing these tumors and judging the mode of removal lies with the infertologist.
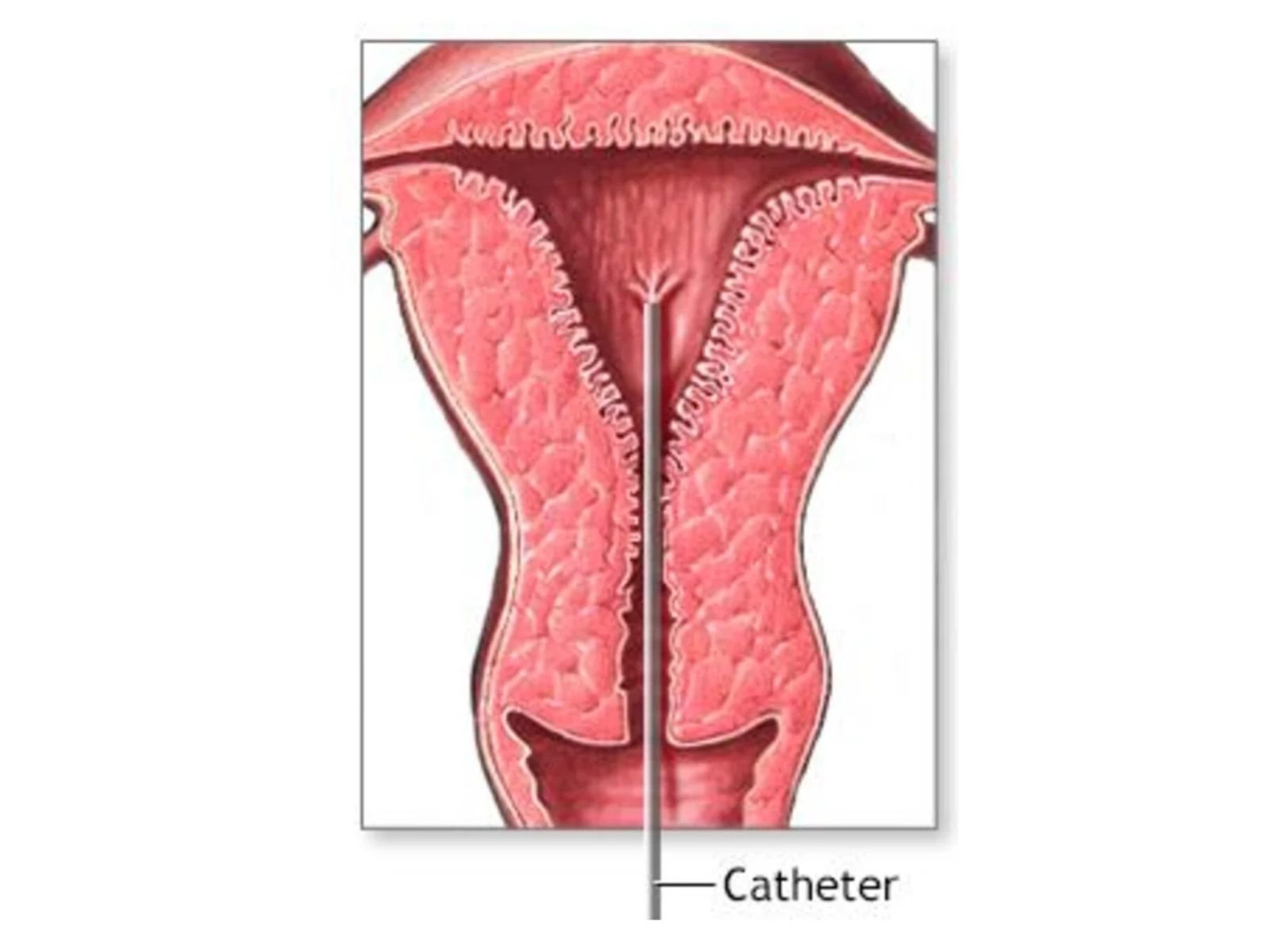
This is a simple procedure done to retrieve a sample of the endometrium (lining of the uterine cavity) for purpose of testing for pathology, especially in cases of abnormal uterine bleeding. It may be done as an office procedure or using a short anesthetic in those cases where there is difficulty in negotiating the cervix which precludes retrieval of an adequate sample.
It is also performed as a part of the diagnostic laparoscopy/hysteroscopy to assess the phase of the uterine cycle. Most often a fractional curettage is performed prior to hysterectomy (removal of the uterus, tubes and ovaries) whereby samples are obtained from both the endocervix and the endometrium.

Cervix biopsy like the endometrial biopsy is used to diagnose any lesion in the cervix. It may be done as an office procedure or in combination with cryocautery where short anesthesia may be required. Cryocautery is done as one of several therapeutic procedures for women with one or more abnormal pap smears. It is especially done in benign cases giving good results. Normally a heavy vaginal discharge is expected following the procedure and abstinence from sexual activity is advised for a period of 10 days. For a better understanding kindly visit the following link.

This is done for patients who have exhibited previous cervical incompetency, demonstrated patulous internal os at diagnostic laparoscopy and/or repeated threatened abortion in current pregnancy. In our center, we perform the procedure at 16 weeks of gestation after ensuring a sonographically normal fetus and absence of chorioamnionitis. Prior to the procedure which is done under general anesthesia, the patient is put on prophylactic antibiotics to prevent any infection and also medications to keep the uterus relaxed (tocolytics). During the procedure 3 sutures are applied antero – posteriorly, thereby closing the mouth of the uterus (Cervix). We have found that it is ideal to do this procedure between 14th to 16th week of pregnancy, since the risk of abortion is higher when done earlier or later than this crucial period. Chronic illness can also lead to excessive bleeding. However the thermal balloon ablation is a technique employed to destroy the endometrium in order to either reduce the bleeding or stop it completely. It can be done as a day care procedure with short anesthesia. It is an alternative to hysterectomy in patients with benign conditions belonging to the younger age group and who have preferably completed their family.
Cervix biopsy like the endometrial biopsy is used to diagnose any lesion in the cervix. It may be done as an office procedure or in combination with cryocautery where short anesthesia may be required. Cryocautery is done as one of several therapeutic procedures for women with one or more abnormal pap smears. It is especially done in benign cases giving good results. Normally a heavy vaginal discharge is expected following the procedure and abstinence from sexual activity is advised for a period of 10 days. For a better understanding kindly visit the following link.
This is done for patients who have exhibited previous cervical incompetency, demonstrated patulous internal os at diagnostic laparoscopy and/or repeated threatened abortion in current pregnancy. In our center, we perform the procedure at 16 weeks of gestation after ensuring a sonographically normal fetus and absence of chorioamnionitis. Prior to the procedure which is done under general anesthesia, the patient is put on prophylactic antibiotics to prevent any infection and also medications to keep the uterus relaxed (tocolytics). During the procedure 3 sutures are applied antero – posteriorly, thereby closing the mouth of the uterus (Cervix). We have found that it is ideal to do this procedure between 14th to 16th week of pregnancy, since the risk of abortion is higher when done earlier or later than this crucial period. Chronic illness can also lead to excessive bleeding. However the thermal balloon ablation is a technique employed to destroy the endometrium in order to either reduce the bleeding or stop it completely. It can be done as a day care procedure with short anesthesia. It is an alternative to hysterectomy in patients with benign conditions belonging to the younger age group and who have preferably completed their family.

These individual conditions exert their own effects on fertility, sometimes necessitating the need for in vitro fertilization (IVF). However research has proven that clearance of these pathologies prior to application of the different modalities of assisted conception significantly improves results. Mostly we perform adhesiolysis, removal of endometriotic cysts in the ovary and the removal of gross hydrosalpinx fluid collection in the fallopian tube laparoscopically. Sometimes when two or more conditions co-exist in the presence of dense adhesions we perform an open surgery.

This is done as one of the therapeutic modalities in treatment of poly cystic ovarian syndrome. Previously a portion of the ovary was resected surgically leading to complications like adhesions and premature ovarian failure. Recently simple electro cauterization of the ovarian surface is achieved laparoscopically leading to better ovulation and pregnancy rates. Normally 5-8 points on each ovarian surface are cauterized. The advantages are shorter recovery and less adhesion formation.
These individual conditions exert their own effects on fertility, sometimes necessitating the need for in vitro fertilization (IVF). However research has proven that clearance of these pathologies prior to application of the different modalities of assisted conception significantly improves results. Mostly we perform adhesiolysis, removal of endometriotic cysts in the ovary and the removal of gross hydrosalpinx fluid collection in the fallopian tube laparoscopically. Sometimes when two or more conditions co-exist in the presence of dense adhesions we perform an open surgery.
This is done as one of the therapeutic modalities in treatment of poly cystic ovarian syndrome. Previously a portion of the ovary was resected surgically leading to complications like adhesions and premature ovarian failure. Recently simple electro cauterization of the ovarian surface is achieved laparoscopically leading to better ovulation and pregnancy rates. Normally 5-8 points on each ovarian surface are cauterized. The advantages are shorter recovery and less adhesion formation.